Invented by Ralf W. Ackermann, Henrik Aspe, Geoffrey S. Gates, Novo Nordisk AS, Mayo Foundation for Medical Education and Research, MAYO MEDICAL VENTURES
Adaptive interactive preceptored learning systems are designed to adapt to the individual needs of each student. This means that the system can adjust the pace and difficulty of the material to match the student’s learning style and level of understanding. This personalized approach to learning has been shown to increase student engagement and retention rates, leading to better academic outcomes.
Remote image monitoring is a key component of this technology. It allows instructors to monitor students’ progress in real-time, providing feedback and guidance as needed. This feature is particularly useful in fields such as healthcare, where hands-on training is essential. With remote image monitoring, instructors can observe students as they perform procedures and provide immediate feedback, ensuring that they are learning the correct techniques and procedures.
The market for adaptive interactive preceptored learning systems incorporating remote image monitoring is vast and growing. It is particularly relevant in fields such as healthcare, where the demand for skilled professionals is high. As the population ages and healthcare needs increase, the demand for healthcare professionals is expected to grow significantly. This presents a significant opportunity for companies offering adaptive interactive preceptored learning systems incorporating remote image monitoring.
In addition to healthcare, this technology is also relevant in other fields such as engineering, aviation, and the military. In these fields, hands-on training is essential for ensuring that students are prepared for real-world scenarios. Adaptive interactive preceptored learning systems incorporating remote image monitoring can provide this training in a safe and controlled environment, allowing students to gain practical experience without the risk of injury or damage.
Overall, the market for adaptive interactive preceptored learning systems incorporating remote image monitoring is poised for significant growth in the coming years. As the demand for skilled professionals in various fields continues to increase, the need for effective training solutions will become more pressing. Companies that can offer innovative and effective solutions will be well-positioned to capitalize on this growing market.

The Novo Nordisk AS, Mayo Foundation for Medical Education and Research, MAYO MEDICAL VENTURES invention works as follows
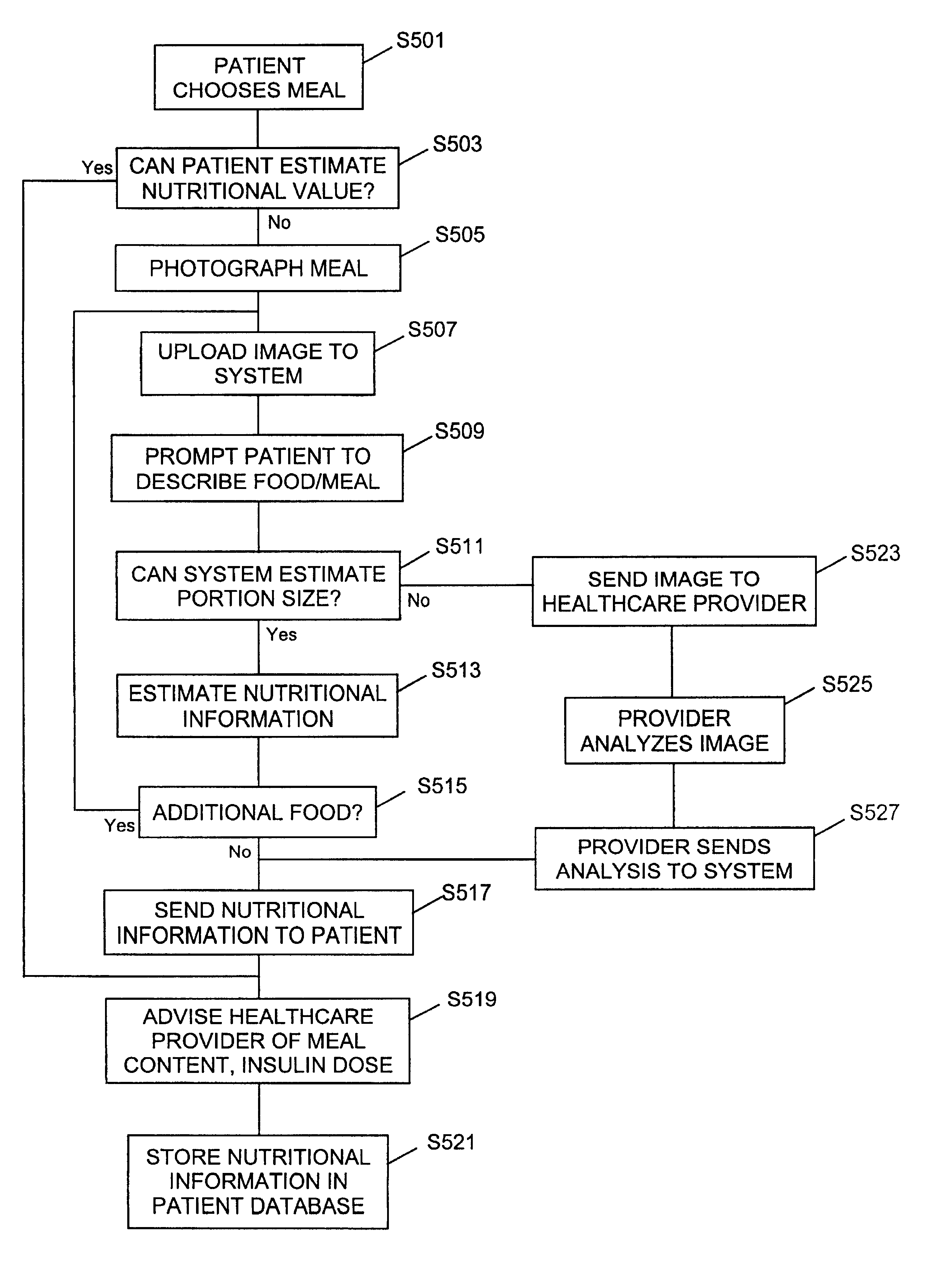
A method of providing an analysis result to a patient that the patient can use to determine the dosage for a self-administration drug when the patient cannot obtain the result themselves. The method includes gathering information by the patient that affects dosage, sending it to an advisor, who analyses the information in order to determine the analysis, sending the result to the client, and then determining the dosage by the client using the analysis. The patient can gather the information by taking a picture of an item of food with a digital camera. The analysis result is the amount of food. The information and the analysis result should be exchanged over the Internet.

Background for Adaptive interactive preceptored learning system incorporating Remote Image Monitoring
The truly curious can always acquire knowledge. Certain formats are more suited to certain goals.
An online encyclopedia, whether it is in CD-ROM or print format, tries to include all relevant knowledge about a topic. An encyclopedia is expected to answer virtually all questions on a subject. An encyclopedia is most commonly used to answer a question and then separate the relevant paragraph or article from the large amount of information. The contents of an encyclopedia are rarely read by users. “In other words, a dictionary does not provide a cohesive educational framework that could guide a student.
Computer format encyclopedias use a variety of strategies to go beyond their limited role in answering questions. The program’s feature articles, which change every time it is launched, are meant to draw the reader to new topics. The encyclopedias can also be used to guide the reader in directions that they would not have found on their own. Encyclopedias are great for answering questions and entertaining the reader, but they don’t document their competence.
A preceptored course (taught) is fundamentally different from an encyclopedia. Preceptored courses are designed to ensure that students who successfully complete the course requirements have a good understanding of the subject. The course might use the resources of a dictionary, but it is directed and arranged by a teacher. “The best teachers take into account the needs of their students when designing a course. However, the overall direction is determined by standards set by experts in order to ensure competence.
Live teaching is not without its drawbacks. The teacher must be paid, a space must be provided for the program and all participants must meet at a designated place.
Another consideration is the limited resources available for live teaching. Dieticians may only have an hour with patients who are being taught to manage diabetes. The dietician might have to use rubber or plastic food models instead of the patient’s meal to teach the patient how to estimate a meal’s nutritional value.
The patient might have to wait longer to see their educator/healthcare professional because the resources are limited. Patients may only see their educator/healthcare providers once every three months to review blood glucose levels. It is important to teach the patient how to handle specific or unique situations. For example, what happens when a patient attends a late-afternoon movie, eats small snacks and then a very late meal. Or, if there are any patterns that arise, like the patient’s blood glucose levels being higher at bedtime when they eat at restaurants instead of home.
Physicians are committed to providing the highest quality care possible to all those who request their services. A comprehensive education is a key component to quality care for someone with diabetes. The limited time available for patients to complete their assessments and the prohibitive cost of individual instruction can make it difficult for physicians to provide high-quality care.
There is therefore a need for a program that combines the advantages of both encyclopedic education and preceptored instruction.
The ongoing treatment of diabetes is one area that is urgently in need of an improved education system. A person with diabetes who has not yet developed symptoms is often asked to change their lifestyle and take multiple medications in order to achieve certain numerical goals. The importance of diabetes education in good diabetes management has been acknowledged. “Diabetes education should provide patients with the necessary knowledge and attitudes to help them accept this challenge.

The primary care provider can improve outcomes by combining an intensive patient education program with the recommended quality measures. Diabetes education can be expensive and difficult to deliver, while the tracking of quality care measures is often lost amongst the busy details of caring for a wide range of patients. “Referring patients to classes in the community, suggesting books or even online diabetes references does not guarantee that each patient will gain the knowledge and skills needed to achieve accepted quality care measures.
An intensification is more likely successful if it is done as soon as a patient becomes motivated to change.” It is important that the education used to inform and motivate the patients is linked directly with the doctors and nurses who can help the patients make changes to their diabetes care.
A course that is precepted with frequent tests and open communication between the teacher and the student ensures that the student will be competent in the subject if he or she completes all the requirements. A patient’s motivation to follow the complicated and burdensome diabetes care requirements can be sustained by frequent communication with an experienced health care provider. However, it is expensive to provide this type of education.
Computer games and interactive education programs for diabetes are not new. No current program combines a precepted course of instruction and the tracking of quality of care measurements from the clinical record of the patient.
There is also a need for a system of interactive and adaptive education that can be used in improving diabetes care.
There is also a need for an interactive Internet-based educational course that can be used as an alternative to one-on-one counseling.
A system is needed to increase the time that a patient with diabetes receives individual education from their healthcare provider.
A system that improves a healthcare provider’s ability to monitor and educate a patient and gives them more time is needed.
As part of the teaching process for managing diabetes, patients learn that the amount of food they consume will determine the amount of insulin they need. According to one school of thought, carbohydrates should account for 50-60%, proteins 20-25%, and fats 20%-30% of total calories. (Carbohydrates break down quickly into glucose during digestion, and therefore have the greatest immediate impact on blood sugar, so it’s better to consume starches and complex carbohydrates than simple sugars and fruit juices. Doctors usually recommend eating three to four small meals every day and a few snacks to keep the balance of glucose and insulin. Patients who are overweight may be encouraged by their doctors to eat less fat and more complex carbohydrates.
A different school of thoughts favors the “Mediterranean” diet, in which some carbohydrates are replaced with monosaturated fats such as olive oil. Diets that replace some carbohydrates with monosaturated oils such as olive are called Mediterranean diets. The present invention can be used to monitor such a type of diet as well as other types of diets.

Patients learn how important it is to accurately calculate the amount of insulin they need to administer by accurately determining their food intake and its nutritional value.

Click here to view the patent on Google Patents.